
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Expert Q&A
Evaluating and Treating Patients With Problematic Sexual Behaviors
 Amos Turner, MD.
Amos Turner, MD.
Assistant professor of clinical psychiatry, Yale School of Medicine, New Haven, CT.
Dr. Turner has no financial relationships with companies related to this material.
CATR: Tell us about your specialty within the field of addictions.
Dr. Turner: I am an outpatient psychiatrist at the VA. I focus on posttraumatic stress disorder, substance use disorders (SUDs), and have a specialty clinic for people who have concerns related to sex, pornography, or other behavioral addictions.
CATR: Sex is a normal part of life for most people. When does it became an addiction?
Dr. Turner: The DSM doesn’t have a diagnosis of sex addiction, and I tend to not use that term very often. The ICD-11 recognizes compulsive sexual behavior disorder, but there is still debate in the field about whether this is the best label. Like many psychiatric disorders, you should consider treatment if the patient is in distress. It may seem simplistic, but sex is worth exploring clinically when a patient tells me it’s having an impact on their well-being. As an addiction psychiatrist, I find it helpful to think of when someone compulsively continues to do something, whether it’s a sexual behavior or substance use, despite negative consequences.
CATR: What term do you use if not addiction?
Dr. Turner: There are a lot of terms; I’ve found that many patients identify with “out of control sexual behavior.” And compulsive sexual behavior disorder is in the ICD-11, so there’s rationale for that. But I have an open and honest discussion and try to mirror the patient’s language whenever possible. If a patient says, “I feel like I’m addicted,” and that’s a useful concept for them, then I’ll use the word “addiction.” I try to stick to language that feels right to them. The caveat is if the language the patient is using is overly negative or judgmental. If so, that can be an opportunity for exploration. Where does that opinion come from, and what does it say about how they feel about themselves? Just like in SUDs, many patients have internalized shame and guilt, and we’re battling negative self-talk. If the language used by the patients seems overly judgmental or self-defeating, I’ll ask, “Is this language helping you achieve your goals, or is it a part of what’s keeping you stuck?”
CATR: Many patients must be reluctant to talk about sex. How do you approach gathering a history?
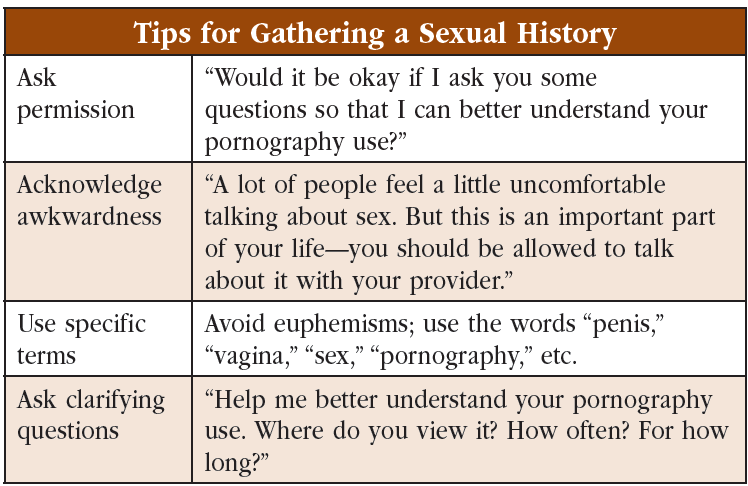
Dr. Turner: I use three techniques to overcome any initial reluctance to talk about sex. First, I ask permission: “Would it be okay if I ask you some more questions so that I can better understand your pornography use?” I do this even if this is the chief complaint and why they are here to see me. Second, I acknowledge that many people are taught that it’s not okay to talk about sex. I tell them it’s normal for it to feel a bit awkward, but I also point out that this taboo doesn’t entirely make sense. I say to them, in a slightly perplexed tone: “Here is this thing that is important to your life (or relationship), and you’re not supposed to ever talk about it at all?!” I think this helps with therapeutic alliance and also enhances motivation by establishing that your relationship and sexual well-being is more important than a little awkwardness. Third, I use specific terms when discussing sex (“masturbation,” “pornography,” “orgasm,” “penis,” “vagina,” etc). This decreases confusion and models that it is okay to discuss sexual topics. It helps patients practice sexual communication that could be helpful in their personal lives as well as appointments with me.
CATR: Any other tips?
Dr. Turner: Ask clarifying questions to fully understand situations the patient is describing. This is very similar to substance use. If someone with alcohol use disorder (AUD) says, “I drank on Saturday,” we would likely ask about the circumstances, triggers, how much they drank, where they drank, how they felt, etc. I think the same thing applies to sexual topics. For example, if someone’s goal is to reduce pornography consumption and they disclose that they viewed pornography recently, I would ask a similar line of clarifying questions so that we can better understand the situation and plan for the future (Editor’s note: See “Tips for Gathering a Sexual History” table). Finally, let the patient lead the conversation and be willing to follow them. The patient will tell you what you need to know if you maintain openness and a nonjudgmental curiosity. People are very good at reading nonverbal cues. Patients respond to our cues, even subconsciously, about what topics are okay to talk about and what topics might be off-limits.
CATR: Any tips on how to maintain this nonjudgmental stance?
Dr. Turner: This is an issue that many providers struggle with. A book that was very influential to me is Treating Out of Control Sexual Behavior: Rethinking Sex Addiction (Braun-Harvey D, Vigorito MA. New York, NY: Springer Publishing; 2016). The authors suggest asking, “What is your vision of sexual health?” This question reorients the treatment toward a goal of improving overall well-being in relationship to sexuality, instead of trying to change specific behaviors. As I said, providing a nonjudgmental space for individuals to explore their sexual beliefs and behaviors is crucial. Of course, that doesn’t mean we should support or encourage literally any sexual behavior. Clearly there are some that should be discouraged—pedophilia, exhibitionism, or any nonconsensual sex, for example. This book proposes six principles of sexual health that I find helpful to keep in mind: 1) consent, 2) nonexploitation, 3) protection from HIV/STIs and unwanted pregnancy, 4) honesty, 5) shared values, and 6) mutual pleasure. If a patient’s sexual behaviors are in line with these principles, we don’t really have standing to discourage them. It’s the combination of keeping these principles in mind along with constantly working toward improving general sexual health well-being that helps me maintain a healthy, nonjudgmental space.
CATR: And how does all this relate to SUDs?
Dr. Turner: There are some aspects that overlap, which I think are fairly obvious. The areas that don’t overlap can pose a particular challenge, though. For example, pornography is involved in most of the referrals I receive. In SUD treatment, one fundamental approach to treatment is to remove access: not keeping alcohol in the house, flushing your drugs, deleting your dealer’s number. But technology has made that approach impossible; people have an essentially unlimited supply of novel sexual content they can access through their phone, which is with them 24 hours a day.
 CATR: What are some other challenging areas that don’t overlap with SUDs?
CATR: What are some other challenging areas that don’t overlap with SUDs?
Dr. Turner: In SUDs, the concept of abstinence or sobriety is pretty well understood. If someone is having medical or personal problems related to cocaine use, the goal is usually to stop using cocaine. But how do you conceptualize sobriety when it comes to sex? Even if sex is a problematic area in someone’s life, the goal might not be complete celibacy. For many, sex and sexuality are an integral part of life. Here, I use a concept from the SUD world: “define your own sobriety” (if they identify with addiction terminology). Work with the patient to come up with their own goals and define what, for lack of a better term, their “best sexual life” might look like. That will look different for everybody because it’s highly personal. Fundamentally, we are trying to cultivate a sex-positive attitude. What I mean by that is we are helping a person explore their sexual behaviors, their fantasies, and their belief systems in order to identify what behaviors promote their sexual health and well-being and what behaviors present barriers to achieving that well-being.
CATR: Can you elaborate on specifically how you do this?
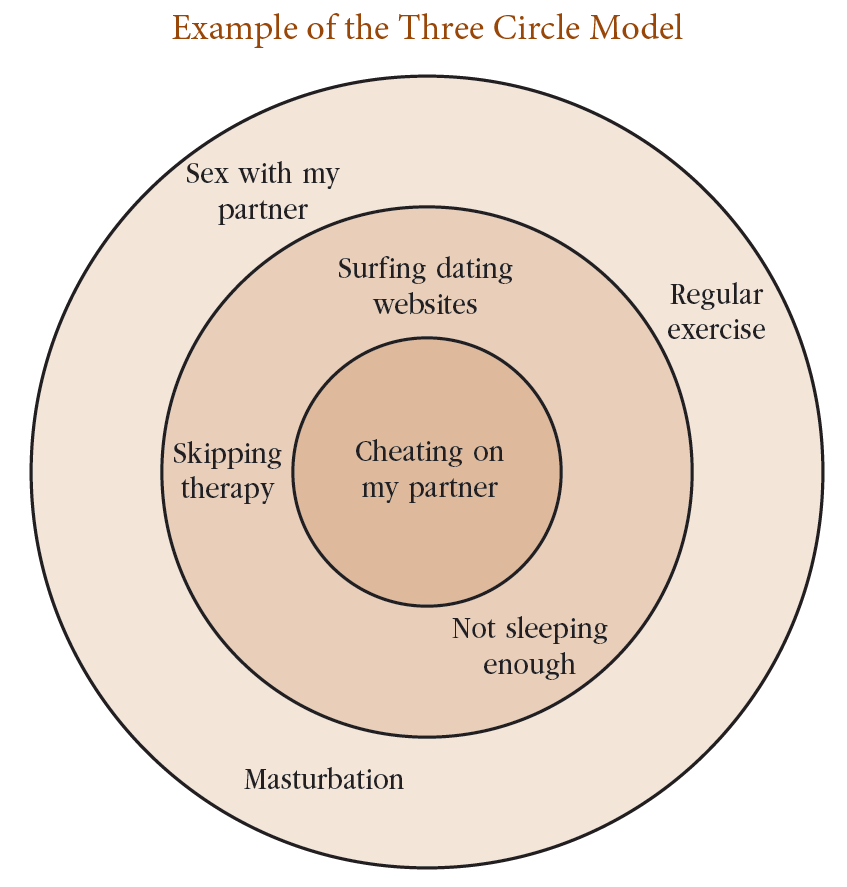
Dr. Turner: I use the Three Circle Model, which comes out of 12-step programs (www.tinyurl.com/37xbzhve). It’s a helpful way of visualizing sexual goals. Imagine three concentric circles, like a bullseye: There’s an inner circle, a middle circle, and an outer circle. On the inner circle are behaviors the person hopes to change. These are behaviors to avoid completely. The middle circle contains behaviors that don’t necessarily violate the person’s sexual health goals, but if they aren’t careful with middle circle behaviors, they might be more likely to engage in inner circle behavior. And the outer circle contains healthy, positive behaviors, both sexual and nonsexual (Editor’s note: See “Example of the Three Circle Model”). For example, the inner circle might have the goal of eliminating infidelity, while the middle circle has behaviors like surfing dating websites. Patients can include nonsexual behaviors in the middle circle too, like skipping therapy appointments or not getting enough sleep. The outer circle might be sex with a long-term partner, masturbation, exercise, or time with friends.
 CATR: Once you’ve defined these goals, what’s next? What are the treatment options?
CATR: Once you’ve defined these goals, what’s next? What are the treatment options?
Dr. Turner: Psychotherapy, mostly rooted in a behavioral approach, has the most robust evidence. This can be offered in group or individual settings. There is evidence for many modalities, including cognitive behavioral therapy, motivational interviewing, acceptance and commitment therapy, and mindfulness-based relapse prevention (Efrati Y and Gola M, Curr Sex Health Rep 2018;10:57–64). For many patients, adding in couples therapy can be beneficial. My personal preference is not to be too dogmatic about any single approach. In my experience, I’ve found that adapting components of various approaches works the best. As I said before, attitudes, beliefs, and desires about sex are highly personal, so a lot of the early work is just helping a person figure out what approach will work for them. What fits with their life? What fits with their culture and belief system?
CATR: How do you suggest a nonexpert go about treating these patients?
Dr. Turner: You can’t expect providers to have expertise in all the modalities I mentioned. But just meeting with a patient, allowing them to express these issues in a nonjudgmental space, can be enormously helpful. Helping them to clarify what, for them, is a problematic versus healthy behavior can be a very meaningful first step as well. Twelve-step groups are widespread and helpful for some. Sex Addicts Anonymous is probably the biggest one, but there are others, each with their own attitude and ethos. Some are online and some are in person. You just need to see what works best for your patient; for some, the 12-step approach may not be a good fit. A recovery phrase that I love is, “Take what you need and leave behind the rest.” I tell patients we’re going to try a lot of things and if something works, they can keep doing it—but if something doesn’t, that’s okay too.
CATR: There are phone apps available as well, right?
Dr. Turner: There are apps for those struggling with issues specifically related to the internet, be it pornography or dating websites. I recommend exploring apps that can help to limit access; there are a lot of them out there, and the landscape is constantly shifting, so I recommend that patients do some research and pick one that fits best for them.
CATR: It sounds like there are a fair number of resources available.
Dr. Turner: Yes, that’s right—which also brings up the importance of a well-rounded team with complementary approaches. An addiction psychiatrist or general psychiatrist can approach sexual issues from a particular standpoint. Peer support groups can be valuable in a different way. Sex therapists, who are very much experts, can also be helpful for patients who have access to them.
CATR: There is some evidence for medication as well, right?
Dr. Turner: Naltrexone has a little evidence (Savard J et al, J Sex Med 2020;17(8):1544–1552). It’s not been studied enough to be the standard of care, but given its favorable safety profile, it’s a reasonable thing to try. I would recommend dosing it just as you would with AUD, the standard being 50 mg daily, with the option to decrease to 25 mg or increase to 100 mg daily. It’s also important to treat comorbid psychiatric issues. This is an opportunity to point out the importance of good dual diagnosis care. Anxiety, depression, and trauma-related disorders are highly comorbid with all types of addictions, including behavioral addictions. This is where antidepressants like SSRIs and SNRIs can be helpful. And actually, the adverse effects of these medications on libido and sexual dysfunction can be beneficial for some patients.
CATR: Any final thoughts?
Dr. Turner: I would just like to pass on encouragement to providers out there who might have discomfort dealing with these issues. To some extent, we all want to stay within our own bubble of expertise. I’m the same way. But remember, when it comes to issues related to sex, you are helping a patient have space to explore something they may never have talked about before in their life. It can be healing simply to get more comfortable talking about sex, saying the word masturbation out loud, describing fantasies—they realize, “I wasn’t judged. This didn’t go horribly. I thought I was going to take this to the grave.” That’s a powerful gift that you can give to your patients, no matter your level of training or area of expertise.
CATR: Thank you for your time, Dr. Turner.


Recommended


