
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Expert Q&A
Deprescribing Benzos: A How-To Guide
 Audrey Abelleira, PharmD, BCPP. Clinical pharmacist practitioner, VA Connecticut Healthcare System; clinical instructor, Yale School of Medicine, New Haven, CT.
Audrey Abelleira, PharmD, BCPP. Clinical pharmacist practitioner, VA Connecticut Healthcare System; clinical instructor, Yale School of Medicine, New Haven, CT.
Dr. Abelleira has no financial relationships with companies related to this material.
CATR: Please introduce yourself.
Dr. Abelleira: I’m a clinical pharmacist at VA Connecticut. My work is at the intersection of chronic pain and substance use disorders, and I operate a benzodiazepine (BZD) deprescribing clinic.
CATR: Why deprescribe at all?
Dr. Abelleira: There are quite a few dangers of chronic BZD use, many that can be catastrophic. For older patients, they increase rates of cognitive impairment and falls. And BZDs are involved in many overdose deaths. A fatal overdose on BZDs alone is rare, but they can have powerful synergistic central nervous system depressant effects when combined with opioids. And even though they are prescribed to treat anxiety, chronic use is associated with worsening of anxiety. In my own work with veterans, I see many BZD prescriptions meant to manage PTSD symptoms, but in fact, the BZD interferes with evidence-based psychotherapy and can be counterproductive (Guina J et al, J Psychiatr Pract 2015;21(4):281–303).
CATR: How widespread are these problems?
Dr. Abelleira: The negative outcomes are so wide ranging that it’s impossible to say definitively. But I think they are more widespread than we generally acknowledge. We do know that many overdose deaths involve BZDs, often in combination with opioids (www.tinyurl.com/ywfzp7m2). And anecdotally, many symptoms that we might associate with aging, like cognitive and memory impairments, or safety in the home, might in fact be due to BZDs.
CATR: What would prompt you to recommend a taper?
Dr. Abelleira: Believe it or not, some patients refer themselves. Maybe they miss a dose and realize how physically dependent they have become or recognize that it is causing them problems. Other times it’s concerns about safety in the home: recent falls or a patient who is seemingly more forgetful. I get referrals for younger patients with PTSD or anxiety who are starting psychotherapy or who require escalating doses to keep symptoms in check. In those cases, you can get some resistance from the patients.
CATR: What do you do when you encounter resistance? Is it common?
Dr. Abelleira: In my experience, about 25% of patients are reluctant to taper even before the first appointment. Others may become resistant after a few dose reductions. But I’ve found it helpful to repeatedly emphasize the tangible benefits of tapering that are relevant to the specific patient. For example, for an older patient who has fallen at home, I stress how getting off the BZD might allow them to live independently longer. For a younger patient, I emphasize how getting off BZDs could improve anxiety. Many patients have been on these medications for decades, so we don’t need to rush. Patients are more amenable if they know the plan is to start small and make little changes. Over time, the little changes will add up. And don’t overlook the importance of simple reassurance. I say “I’m here to work with you, not force you to do something you’re not ready to do. If a change doesn’t go well, you won’t be left high and dry.”
CATR: What about patients with symptomatic anxiety?
Dr. Abelleira: Many patients with anxiety disorders who are on BZDs still suffer severe anxiety symptoms. So I highlight the paradox—the BZD is supposed to be helping, but not only is it ineffective, it’s dangerous as well and is probably making the anxiety worse.
CATR: How do BZDs worsen anxiety?
Dr. Abelleira: It’s an important question that likely has several answers. Like many medications, patients develop tolerance and therefore can have rebound anxiety between doses as part of a withdrawal syndrome. Additionally, there are hypotheses that worsen anxiety by disrupting the hypothalamic-pituitary-adrenal axis, which is important in stress regulation, and causing changes to serotonergic neurotransmission. BZDs interfere with fear extinction as well. So, although it may seem counterintuitive, chronic BZDs do tend to worsen symptoms of generalized anxiety, phobias, and PTSD over the long term (Guina J and Merrill B, J Clin Med 2018;7(2):17).
CATR: Let’s talk about some strategies. How do you start a taper?
Dr. Abelleira: Generally, I’m working with patients who have been prescribed BZDs for many years. They have a high level of tolerance and can be very sensitive to dose reductions. So, the strategies I am laying out apply to this patient population specifically. Usually, I won’t do an initial dose reduction of more than 25% at the first visit. Sometimes I taper by as little as 10% at first.
CATR: How do you know where to start?
Dr. Abelleira: All things being equal, I taper high doses a bit slower. It also depends on the agent; patients on BZDs with a long half-life can usually tolerate a larger decrease than those on a drug with a short half-life. Of the commonly used BZDs, alprazolam is the short-acting one. Diazepam is very long acting. Lorazepam is in the middle. Clonazepam is also in the middle, but I find that it leans more long acting. Clonazepam, lorazepam, and diazepam tapers are usually straightforward. Alprazolam tapers are the most challenging for patients to complete.
CATR: Where do you go after that first dose reduction?
Dr. Abelleira: I will usually plan on another dose reduction in two to four weeks at the same percentage of that initial drop. But these are general principles; it really depends on how that first drop goes. For example, if we start at 25% and that goes well, we’ll decrease by that same amount every two to four weeks until the patient is off BZDs completely. On the other hand, if the 25% does not go as hoped, the next step might be 10%–15%. I try not to predetermine the course of the taper ahead of time. I’m open to changing course mid-taper.
CATR: Do you ever switch agents?
Dr. Abelleira: I do, typically after I’ve made a few dose reductions of a shorter-acting BZD and we’re getting stuck. In those situations, I’ll switch to diazepam, which is very long acting. Diazepam is also helpful at the end of a taper when we’ve gotten down to the smallest available dose of a shorter-acting BZD but the patient is not quite ready to stop. That’s usually 0.125 mg of alprazolam or 0.25 mg of lorazepam or clonazepam.
CATR: Do you switch the other way: from long acting to short acting?
Dr. Abelleira: I prefer that frail elderly patients not be on diazepam. Their cognition can be sensitive to a lingering drug in their system. The long half-life, lipophilicity, and active metabolites of diazepam mean it’s not a good choice for them. Lorazepam is a good choice in that situation, though it needs to be dosed more frequently. I’ll find an equivalent dose, halve it, and prescribe it to be taken twice daily. It’s not an exact science and sometimes it needs adjustment, but this is a good place to start.
CATR: How do you do that switch?
Dr. Abelleira: Most of the time I just do a direct switch. I’ll calculate an equivalent dose, stop one, start the other, monitor the response, and adjust if needed. Sometimes I’ll do a brief overlap when the patient is switching off alprazolam. The fast onset of alprazolam can be very reinforcing, and other agents may not give that same immediate relief. “It’s just not working; I can’t tolerate this” is a frequent response if alprazolam is stopped too quickly. In those cases, I’ll start with a cross-taper to a longer-acting BZD, usually diazepam. It’s rare that the overlap needs to be more than a couple weeks.
CATR: What resources would you recommend for BZD dose equivalencies?
Dr. Abelleira: The standard is to convert everything into lorazepam equivalents (Editor’s note: See “Benzodiazepine Equivalencies” table ). There are a few established guidelines as well as online calculators, which can be handy (www.tinyurl.com/2p8euwxx; www.tinyurl.com/ywdyw44j).
CATR: Do you worry about cross-tolerance?
Dr. Abelleira: I typically go one-to-one and don’t worry about cross-tolerance. But it isn’t always exact, and some references will give you slightly different numbers. This means it is important to closely monitor the patient after making the switch so that you can adjust accordingly.
CATR: How long can these tapers last? Months? Years?
Dr. Abelleira: It can take months. For me, the average is about six months, rarely more than a year. It can be a long process, but remember that many of these patients have been taking BZDs for many years, often decades. A year is a drop in the bucket.
CATR: What patient characteristics lead you to think that a longer taper might be necessary?
Dr. Abelleira: Patients with poorly controlled anxiety usually need slower tapers, as do patients who are resistant to the idea of tapering to begin with. Even when everything else is stable, I’ll start with a more gradual taper for these patients so that they have a positive initial experience. Each dose reduction that goes well is an opportunity for the patient to see that they can be successful, get to know me, and trust that I’m not going to expect them to do something unmanageable.
CATR: Are longer tapers required for patients who have been on BZDs for a long time?
Dr. Abelleira: You hear that all the time, but I’m not convinced this is entirely true; there isn’t hard research to say one way or another. These are all tolerant patients, so does a treatment history of five years versus 10 or 15 years really make a difference? I’ve seen providers scared to reduce BZD doses because of a long treatment history and become overly cautious—a miniscule dose reduction every six months. It’s unnecessarily long and sends the message to the patient that this is some big undertaking. I’ve had patients get fed up and say “I can’t even talk about this anymore. Just leave me alone.”
CATR: What signs and symptoms are you looking for as a taper progresses?
Dr. Abelleira: I’m looking for subjective increases in anxiety and trouble sleeping, specifically new-onset insomnia. A common physical sign of BZD withdrawal is a fine tremor. A little bit of discomfort is common, but it should be tolerable. We monitor vital signs at every visit, and you can see elevations in pulse and blood pressure, though not commonly. Vital sign abnormalities are much more common in those stopping BZD cold turkey.
CATR: Do you ask patients to monitor their vitals at home?
Dr. Abelleira: I don’t. Some patients with hypertension monitor it already, and I don’t discourage that. But we shouldn’t be seeing dangerous elevations with these slow, controlled tapers, so it’s not medically necessary. And these patients are generally anxious already, so if I give them an objective measure that they can check all the time, I find that some can hyperfocus on it. Any slight abnormality can be upsetting despite having zero clinical relevance.
CATR: How do you manage the increased anxiety?
Dr. Abelleira: If a patient is not already on an antidepre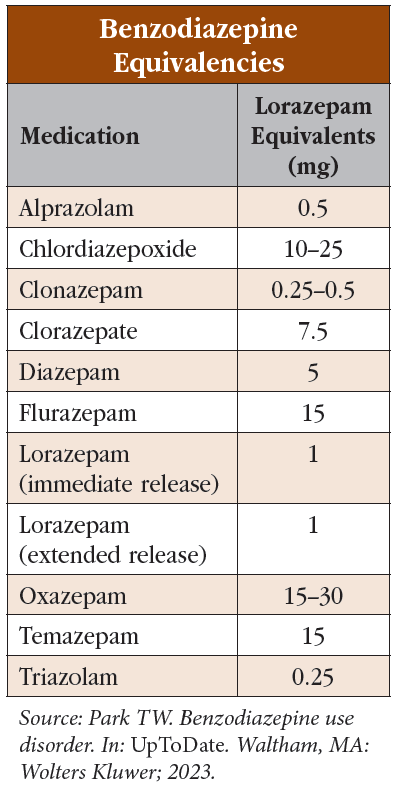 ssant, I’ll start an SSRI and titrate it as we taper the BZD. For breakthrough anxiety, I utilize non-BZD alternatives; 25–50 mg of hydroxyzine several times a day can be helpful for some. If hydroxyzine isn’t helpful or not an option, I’ll try a low dose of propranolol starting at 10 mg three times a day.
ssant, I’ll start an SSRI and titrate it as we taper the BZD. For breakthrough anxiety, I utilize non-BZD alternatives; 25–50 mg of hydroxyzine several times a day can be helpful for some. If hydroxyzine isn’t helpful or not an option, I’ll try a low dose of propranolol starting at 10 mg three times a day.
CATR: What about for insomnia?
Dr. Abelleira: I’ll use factors specific to each patient to inform which non-BZD sleep medication I choose. If they have depression, mirtazapine is a good choice, or doxepin if they have chronic pain. Trazodone is not recommended in most insomnia guidelines, but that can be an option as well, typically second or third line.
CATR: Do you ever use Z-drugs?
Dr. Abelleira: I try not to. In some cases, the safety concerns of Z-drugs and BZDs are similar. For instance, if we’re tapering the BZD for an elderly patient, switching to a Z-drug doesn’t necessarily mitigate fall risk or cognitive impairment. However, it is less clear-cut whether Z-drugs increase opioid overdose risk, and they are probably safer than BZDs, so that might be a reason to use a Z-drug.
CATR: Are there patients that just can’t get off BZDs?
Dr. Abelleira: Sometimes, yes; maybe about 20% of my patients fall into that category. But keep in mind I’m generally seeing the most challenging cases. For those patients, we get them as low as possible. We optimize pharmacotherapy for the diagnosis that prompted the BZD prescription in the first place and mitigate risks as best we can in other ways. Trying to force a patient to fully discontinue a BZD when they are really distressed is not going to result in a positive outcome. And the door is always open to try again.
CATR: What other ways might you mitigate risk?
Dr. Abelleira: If somebody is on opioids and we can’t get them off the BZD entirely, maybe we can reduce the opioid instead and lower risk that way. For our elderly folks, are we able to limit polypharmacy, specifically for anticholinergics? If falls are a concern, referral to occupational and physical therapy can help. Simple interventions like home safety should not be neglected. These are the sort of risk mitigation strategies that we should be thinking about for all our patients, but they become especially important if we aren’t able to completely discontinue the BZD.
CATR: Is there anything else you’d like to mention?
Dr. Abelleira: I’ll just add that the BZD deprescribing clinic is my favorite part of the week. Patients have been on these medications for so long that many feel like it’s impossible to come off them or reduce the dose. And when they start to have success and they start to realize they can do this, they are so proud of themselves. They are so excited. Many providers dread addressing this topic with patients, but I’d say most of the time, it’s a very positive and rewarding experience for both me and the patient.
CATR: Thank you for your time, Dr. Abelleira.


Recommended


