
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Clinical Update
Confused About Acute Confusional States? A Primer on Delirium
Delirium is one of the most serious problems facing hospitalized patients. It nearly doubles a patient’s risk of death and often produces irreversible cognitive and functional impairment (Wilson JE et al, Nat Rev Dis Primers 2020;6(1):90). It is extremely common, occurring in approximately one in five inpatients, with even higher rates among patients in surgery units and ICUs (Burton JK et al, Cochrane Database Syst Rev 2021;11(11):CD013307). Despite the high prevalence, more than half of delirium cases go undetected. In this article, we will review key points in the diagnosis, workup, and management of this acute confusional state.
Clinical features
“Delirium” describes an acute change from baseline mental status marked by inattention, disorientation, and thought disorganization (see “DSM-5 Delirium Diagnostic Criteria” box). Symptoms fluctuate over the course of a day, and patients often appear fully lucid for brief periods. Their sleep-wake cycles are disturbed, and they may demonstrate a broad range of emotions or experience hallucinations (Inouye SK, N Engl J Med 2006;354(11):1157–1165). Other terms often used to describe delirium include encephalopathy, altered mental status, and acute confusional state. However, these terms are not considered synonymous, and the term delirium is preferred when referring to clinical features observed at the bedside (Slooter AJC et al, Intensive Care Med 2020;46(5):1020–1022).
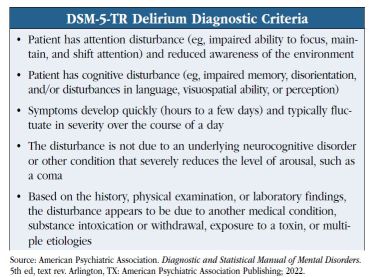
Box: DSM-5-TR Delirium Diagnostic Criteria
(click to view full size PDF)
Delirium is classified as hypoactive, hyperactive, or mixed. Hypoactively delirious patients may go unnoticed, as they are withdrawn and may appear to be quietly resting. When we receive a consult for “depression,” we make sure to evaluate the patient for hypoactive delirium. A hyperactively delirious patient, on the other hand, requires a great deal of attention on the medical/surgical floors. These patients are agitated and hypervigilant, and often are combative or refuse care. We consider a consult for “psychosis” or “mania” to actually be a hyperactively delirious patient until proven otherwise. Patients in a mixed delirium alternate between the hypoactive and hyperactive states.
Who is most at risk?
A history of delirium, advancing age (>65 years), preexisting cognitive impairment or dementia, polypharmacy, and underlying medical illnesses are particularly important predisposing risk factors (see “Risk Factors for Delirium” table). Precipitating factors are triggers that contribute directly to the onset of delirium. These include medication use (eg, anticholinergics, opioids), acute medical illnesses (eg, meningitis, sepsis, stroke), surgery, dehydration, physical restraints, alcohol or drug withdrawal, and prolonged sleep deprivation. The greater the number of risk factors, the greater the risk for delirium.
 Table: Risk Factors for Delirium
Table: Risk Factors for Delirium
(click to view full size PDF)
Identifying delirium
When we are asked to evaluate a potentially delirious patient, we speak with the covering provider and conduct a thorough chart review, looking at vital signs, labs, and medications, with a particular focus on recent changes or trends.
When we go into the patient’s room, we start with basic questions regarding the patient’s comfort in the hospital, food intake, etc, while we attempt to build rapport. These questions also help us to assess the patient’s level of alertness and overt cognitive impairment as well as distrust or paranoia. Patients are often poor historians, so collateral history from nursing staff, physical or occupational therapists, and family is useful. We ask, “Is this patient more confused than before?”
Delirium’s fluctuating course often complicates the diagnosis. Patient presentation varies over hours or days, with the person “at baseline” for one provider only to be somnolent, disorganized, or wildly confused for the next. Repeat evaluations are critical. The following tools improve delirium screening and diagnosis (Mattison MLP, Ann Intern Med 2020;173(7):ITC49–ITC64):
- Confusion Assessment Method (CAM). This is the most widely used delirium tool worldwide, with sensitivity and specificity both >90% and high inter-rater reliability. We sometimes use a shortened version: the 3-Minute Diagnostic Assessment CAM (3D-CAM). For critically ill patients in ICUs, we use the CAM-ICU. (See https://www.thecarlatreport.com/ext/resources/2023/02/09/confusion_assessment-method_cam.pdf)
- 4 A’s Test (4AT). A brief (<2 minutes) validated screening instrument available in multiple languages and requiring no special training for use, though with slightly lower sensitivity (90%) and specificity (84%). The four A’s are Alertness, Attention, Abbreviated Mental Test 4 (AMT-4), and Acute change. (See:https://www.thecarlatreport.com/ext/resources/2023/02/09/4as.pdf)
- Other suggested tests of attention. Ask the patient to spell “world” backwards, subtract serial 7s or 3s, repeat a span of digits (up to five forward or four backward), or recite the days of the week or the months of the year in reverse order.
Identifying causes
The initial workup consists of a physical and neurological exam, review of vital signs, medications (new and/or recently discontinued), and alcohol or drug use. We also examine for possible infectious, metabolic, or electrolyte issues and make sure to explore life-threatening causes of delirium: Wernicke’s encephalopathy, hypoxia, hypoglycemia, hypertension, hyper/hypothermia, intracerebral hemorrhage, meningitis/encephalitis, poisoning, and status epilepticus. When available, we look for any clues in nursing notes and flowsheets documenting pain, bowel or bladder function, and any indication of recent malnutrition or dehydration.
Prevention and treatment
Nonpharmacologic and multicomponent (meaning three or more interventions) strategies are extremely effective, reducing the incidence of delirium by over 40% in non-ICU patients (Burton et al, 2021). Below are the 10 most helpful strategies, with the first two being particularly important
(Oh ES et al, JAMA 2017;318(12):1161–1174):
- Orientation and cognitive stimulation. Provide lighting, signs, calendars, and clocks. Reorient patients to time, place, person, and your role. Introduce cognitively stimulating activities, such as reminiscing. Facilitate regular visits from family and friends.
- Sleep enhancement. Avoid medical or nursing procedures during sleep if possible. Schedule medications to avoid disturbing sleep. Reduce noise at night. We strongly encourage the use of melatonin (1–5 mg PO at bedtime) or ramelteon (8 mg PO at bedtime) to help maintain regular sleep in the hospital.
- Early mobilization. Encourage early postoperative mobilization and regular ambulation, and always keep walking aids nearby, such as canes or walkers. Encourage active, range-of-motion exercises.
- Hydration. Encourage patients to drink, using parenteral fluids if necessary. Seek advice regarding fluid balance in patients with comorbidities such as heart failure or renal disease.
- Infection prevention. Look for and treat infections. Avoid unnecessary catheterizations. Implement infection control procedures.
- Nutrition assistance. Seek advice from dieticians. Ensure proper fit of dentures.
- Oxygenation status. Assess for hypoxia and oxygen saturation.
- Pain management. Assess for pain, especially in patients with communication difficulties. Begin and monitor pain management in patients with known or suspected pain.
- Psychoactive medication review. Review medication list for both types and number of medications.
- Vision and hearing. Resolve reversible causes of impairment and ensure hearing and visual aids are available, working, and being used by patients.
If patients become delirious despite these interventions, we nevertheless continue them to prevent worsening of the delirium.
Treating agitated delirious patients
The first-line treatment for delirium always involves promptly addressing underlying medical causes, once identified. Meanwhile, agitated patients with hyperactive or mixed delirium may not respond to attempts at verbal redirection or nonpharmacologic strategies. Antipsychotics are the most widely used class of medications for delirium treatment, although none are FDA approved for this purpose, and studies to date have demonstrated little to no effect on mortality or on delirium duration or severity (Burry L et al, Cochrane Database Syst Rev 2018;6(6):CD005594; Wilson et al, 2020).
So, is there any reason to use antipsychotic medications for delirium? They can be very helpful for patients who: 1) are acutely agitated and at risk of harming themselves or others; 2) are distressed, often due to severe anxiety or psychotic symptoms such as paranoia or hallucinations; and 3) have not responded to attempts at verbal redirection or other behavioral strategies.
We tend to use both typical and atypical antipsychotics, with the specific choice of medications guided by availability, routes of administration, and nursing and medical staff familiarity (see “Pharmacologic Strategies: Severe Agitation in Delirious Patients” table). For most patients, we start with the gold standard of haloperidol IV as needed (in cardiac-monitored settings, given the risk of QT prolongation and torsades de pointes), with a dosage of 0.5–5 mg based on the patient’s age, size, and severity of agitation. If the initial dose is ineffective after 20–30 minutes, subsequent doses can be doubled until the patient is calm. In older patients, we start with a lower dose of antipsychotic, and use particular caution in patients with Parkinsonism, HIV-associated dementia, or evidence of Lewy body disease (in these cases we usually go to olanzapine, with a dose of 2.5–5 mg that can be given IM or in a dissolvable oral form if needed). If there is any concern for active or recent neuroleptic malignant syndrome, antipsychotics should be avoided entirely. We recommend obtaining a baseline ECG to assess and trend QTc when using antipsychotics. In emergent situations this is often not feasible, so the risk of QT prolongation is weighed against risks to patient or staff safety.
 Table: Pharmacologic Strategies: Severe Agitation in Delirious Patients
Table: Pharmacologic Strategies: Severe Agitation in Delirious Patients
(click to view full size PDF)
Given their potential sedative effects, using antipsychotics to manage agitation may provide teams with a false sense of reassurance that the delirium has been effectively “treated,” while medical issues continue unaddressed and the patient presentation shifts to a more hypoactive delirium, with associated morbidity and mortality (eg, aspiration, immobility).
If antipsychotics are contraindicated (eg, in the setting of significant cardiac comorbidities or QT prolongation), we prefer valproic acid as an initial alternative, starting at 125–250 mg three times daily. It can be administered IV (which we have found helpful in highly agitated patients) and may yield additional benefits for patients with delirium in the setting of dementia, traumatic brain injury, or history of mood disorder. Other options are the alpha-2 agonists dexmedetomidine or clonidine 0.1–0.2 mg every six hours (particularly when transitioning patients from dexmedetomidine into non-ICU settings). Dexmedetomidine had been limited to IV infusion in emergency rooms or ICUs, but the FDA’s recent approval of a sublingual formulation (Igalmi—see callout box) is likely to expand its use to additional settings, such as medical and psychiatric inpatient units. Given the association of benzodiazepines with worsening delirium, we reserve their use for delirium secondary to alcohol or sedative/hypnotic withdrawal. Trazodone, starting at 25–50 mg at bedtime, can be helpful in targeting agitation as well as sleep cycle disturbances.
CARLAT VERDICT
Delirium is common yet frequently missed condition in hospitalized patients. It's linked with functional and cognitive decline and a significantly elevated risk of death. Nonpharmacologic multicomponent interventions, such as cognitive stimulation, frequent reorientation, and sleep enhancement, are highly effective in preventing its onset. Use medication sparingly, primarily to keep patients and staff safe and to help patients be more comfortable, while you work to identify and treat the underlying cause.


Recommended


