
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
CLINICAL Q&A
Using Motivational Interviewing in Your Practice
CATR: What are the basic components of motivational interviewing?
Dr. Rosengren: At its most basic, it is a conversation in which you are trying to help someone deal with ambivalence that prevents them from acting on a problematic behavior. It’s really about helping them sort through this ambivalence and come to a decision that makes sense within their framework. At a more complex level, it has to do with things like paying attention to how the patient talks and what kind of language they’re using. It also involves responding differentially—giving less attention to certain kinds of language and more to others—in the service of helping them work through ambivalence.
CATR: So we have a patient who is doing something unhealthy and they come to us for help. But oftentimes they are not certain that they’re ready to give that up, correct?
Dr. Rosengren: Right. There’s something going on, and they want whatever is bothering them to go away. But it doesn’t necessarily mean that they’re ready to make a change. When I first got into the addiction field, one of my mentors would say, “When people come into treatment, they are ready to give up the consequences of the alcohol or drug use, but not the drug itself.”
CATR: So how do we get into that conversation?
Dr. Rosengren: According to the latest edition of Miller and Rollnick’s book, Motivational Interviewing, there are four processes to think about as we are talking with our patients: engaging, focusing, evoking, and planning (Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. New York, NY: Guilford Press; 2012). Starting with engaging is important because this is where we form the connection with patients so they feel they are in a safe place where they can talk about what’s going on in their lives.
CATR: I think most psychiatrists would feel fairly comfortable with the need for engaging and forming an alliance. A patient will come in, and before jumping into asking about symptoms we’re going to say, “How have you been doing; what have you been up to?” etc.
Dr. Rosengren: Yes, but I would add one thing: It’s important to open those conversations with a positive focus. When patients come in and we start asking questions about what’s been happening, what problems have you had since I saw you last, we’re asking people to talk about the negative. If we start with positive things, it opens them up, broadens their focus, elicits positive emotions, and also makes them more willing to talk about areas that aren’t going so well. So what I do with folks is ask about what’s been going well since I saw them last. “Where have you felt successful? Tell me about a time where you experienced happiness, joy, or a moment of awe.” It doesn’t have to be anything big. “What made you smile in the last 24 hours?” Now if somebody’s got chronic depression, that may not be the best question, but then you might start with, “When did you feel a moment of contentment in the last week?”
CATR: Interesting. So we can really be very explicit and say, “I’d like to start today with some of the positives. Tell me about something that you enjoyed since we last talked.” And they may tell you about a great meal that they had or that their baseball team won a big game. How significant is it to bring that kind of positive energy into the mix?
Dr. Rosengren: What the research would say is it starts to change what’s going on at a hormonal level. Barbara Fredrickson, who is a leading thinker in the area of positive emotions, would say there is an opening up of the visual field and that we literally see more when we are experiencing positive emotions. People begin to see connections in things they wouldn’t otherwise see. And the positive emotions allow them to build bonds and connections with others, and thereby build resilience when the difficult times come. She puts it in the context of the evolutionary theory of emotions: Negative emotions serve to protect us in the moment, and positive emotions serve to broaden and build our resources for when stressful times come. And let’s face it, when we talk about what has been going wrong in our life, that’s a stressful sort of conversation (Fredrickson B. Positivity. New York, NY: Crown Books; 2009).
CATR: Okay, that makes sense. You mentioned earlier that there are four phases of motivational interviewing, and that engaging is the first phase. Can you talk about the focus phase?
Dr. Rosengren: There are different ways to find the right focus for a session. We’re all busy, and we don’t have unlimited time to spend with patients, so I find it useful to have a piece of paper that you use to plan the agenda with your patient. I will write down the common things that we tend to talk about. I’ll say, “Let’s look at the page here. Given the amount of time we have today, what do you want to focus on?” This is useful, because it’s a way to focus their attention and it’s a way to focus our attention. It also allows us to more gracefully introduce difficult subjects that we may need to talk about. For example, in addiction work, you might have a positive urinalysis that you need to talk about. You can put that on your menu of options and say, “So one of the things I need to talk about is your UA results.” And then once we have our agenda, I say, “So where would you like to begin?”
CATR: What else do you put on your agenda menu?
Dr. Rosengren: It depends on the type of patient, but for addictions the list will typically include work, family relationships, stress management, cravings, meeting attendance, and fun. I always like to put fun on the list because it’s one of those things that people don’t usually focus on, and yet we know how important it is that patients are creating opportunities to have enjoyable things happen in their lives. I typically draw circles on a sheet of paper, and I put the words in different circles. I also leave a couple of circles blank and say, “These circles are for things that you feel are important to talk about that aren’t on here.” You can also use a simple checklist, but I find the visual effect of circles to be more engaging.
CATR: What about giving the list to patients before they come into the session?
Dr. Rosengren: That can work well. Patients can get into a routine of completing it in the waiting room. Someone can greet patients in the waiting room and hand them out, or you can leave a stack there. There is actually some research to suggest this can prime patients to do good work once they get into session.
CATR: After focusing comes the evoking phase?
Dr. Rosengren: Yes, and this is really where the art of motivational interviewing comes in. You listen for what sorts of change statements that people are making. In MI, we put everyday language into three different categories: change talk, neutral talk, and sustain talk. Change talk means patient statements in favor of the possibility of change. The two subcategories of change talk are preparatory change talk and mobilizing change talk. During preparatory change talk, people say they’re thinking about the possibility of change, but aren’t necessarily ready to move on it yet. You will hear things like, “Yeah, I think my life would be better if I did something about this.” That is a desire statement. Or they may say, “Well, if I made up my mind, I think I could do it.” That’s an ability statement. Or they might say, “Things are just getting worse and worse, and so I can’t continue doing what I’m doing.” This would be a need statement, where you hear about a negative consequence that impels people towards change. On the other hand, a reason statement is more positively framed; for example, “If I stopped going to the bar, I’d have money to spend on some of the things I’d like to do in the long term.”
CATR: This is fascinating; there’s a whole linguistic world out there that we can tune into. All these statements are examples of preparatory change talk, but I suppose we want to hear more mobilizing talk, is that right?
Dr. Rosengren: Both are important. Preparatory change statements do predict change for patients, but studies have shown that mobilizing language tends to predict change more strongly. Mobilizing language has three parts (Moyers TB et al, Alcohol: Clin Exp Res 2007; 31(Suppl 3):40S–47S) (Moyers TB et al, J Consult Clin Psychol 2009;77(6):1113–1124). There’s commitment—people saying, “Yup, I’m gonna do it,” or, “I’m done with it,” or, “I’m not doing it anymore.” Those are all active statements about what people are going to do, and that predicts change well. The second category is activation, which is saying, “I’m ready” or, “I’m willing to do something.” It’s not quite the same as commitment, but it indicates that people are on that path. And the third is taking steps, which is when people are beginning to experiment with the behavior. I refer to this as the “health club phenomenon” where you’ve made your New Year’s resolution to get fit and joined the health club. You go once or twice. It’s a good thing, but you’re not exercising regularly; you’re just experimenting with it. These kinds of statements are all indicative of change talk.
CATR: We’ve gone through the different kinds of change talk, and the point here is that we should be keeping our ears open for these kinds of statements because they bode well. But when we hear them, what should we do? Reflect back on them? Encourage them?
Dr. Rosengren: We should do both. Reflective listening is a particularly effective way to encourage further talk about change. There is research showing therapist behavior influences the appearance of change talk, and change talk begets more change talk (Barnett E, Psychol Addicti Behav 2014;28(4):1212–1219).
CATR: Can you describe the other kinds of statements we should be listening for?
Dr. Rosengren: The flip side of change talk is sustain talk—all the reasons why people want to maintain the status quo or why change is too hard for them. Neutral talk means statements that are neither for or against change. You’re finding out about your patient’s family life and they are telling you about their kids and their partner and those kinds of things. It’s neither for nor against change—just neutral information. But it can quickly become change talk. For example, the person is telling you about last week when they went to the local baseball game. At that point it’s fairly neutral. But then they may say, “Well, I didn’t have a beer, which is normally what I would do.” That’s change talk, and you can follow up with a reflective statement or question, like, “And when you chose not to have that beer, what was going through your mind?”
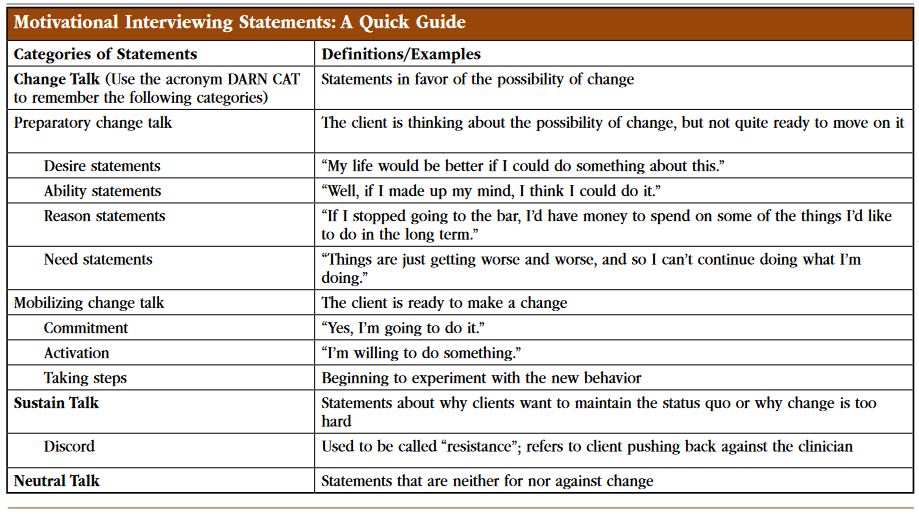 Motivational Interviewing Statements: A Quick Guide: Click here for a larger view of the table
Motivational Interviewing Statements: A Quick Guide: Click here for a larger view of the table
CATR: That makes sense.
Dr. Rosengren: Finally, there is a kind of sustain talk called discord, which used to be called “resistance.” Discord happens when we start pushing on sustain talk to try and get people to change their behavior more quickly—when we push on a patient’s initial ambivalence and the patient pushes back. For example, if a patient isn’t taking their medication regularly, it might be easy for us to say, “You’re not going to get the benefits if you don’t take the medication consistently.” And then the patient says, “Yeah, but then I get side effects I don’t like, so I’m only going to take it when I need it.” We want to avoid statements that are going to elicit more sustain talk. When I’m training counselors, I often say that discord isn’t a patient problem; it’s our problem because it’s about us pushing on them.
CATR: That’s a useful way of looking at the statements a patient could make. Are you suggesting that in most of our sessions we should be thinking in these terms—thinking of categorizing statements in these buckets?
Dr. Rosengren: I would say yes. What we want to do is tune our ears to hear what our patients say and allow that to guide us, especially when we hear weak change talk.
CATR: What do you mean by weak change talk?
Dr. Rosengren: A patient says something like, “So I really don’t think this is all that big a deal.”
CATR: But that sounds more like sustain talk, like they’re not interested in making a change.
Dr. Rosengren: You can read it that way. But there’s also a change element within that statement. The patient’s not saying the issue isn’t a problem; they are just saying the problem’s been overblown by other people. So the art of motivational interviewing involves hearing that little element, and paying more attention to that compared with other parts of the statement.
CATR: It sounds like things can get pretty complicated, but I guess during the actual conversation you’re getting a feel for where a patient is going with these statements.
Dr. Rosengren: When our work with patients is going well, there’s energy and movement. What we’re trying to do with motivational interviewing is direct that movement in a way that’s likely to be productive. We want to help the patient achieve what they want to achieve, and align our goals with theirs. That doesn’t mean we don’t disagree with patients, but we’re trying to figure out their agenda and see if we can get our agenda to work well with theirs.
CATR: What happens when we have a really resistant patient—one who doesn’t want see us at all? How are we supposed to get our agendas in sync?
Dr. Rosengren: That can be tough, but a good way to approach such patients is to identify one of their goals and try to align with it, even if it seems contrary to yours. I’ll give you an example from my previous work with adolescent boys. In 15 years, I never had even one who actually wanted to be in treatment; it was always because so-and-so sent them, and their typical “goal” was to stop seeing me. So I would ask these kids, “What do you have to do to not see me anymore?” We’d figure that out, and it would boil down to something like how did they need to change in order to get their parents off their backs. For folks who are coming in for addiction, your probation officer is on your back; your spouse is on your back; you’re about to lose your job—so what do you have to do in order to be able to keep your job, and how does the alcohol or drug use fit into that? Those are the kinds of questions to ask, and which will help you to agree on goals and get your patient motivated.
CATR: That’s helpful advice. Thank you for your time, Dr. Rosengren.


Recommended


