
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
CLINICAL UPDATE
Four Evidence-Based Psychotherapies for PTSD
Learning Objectives:
After reading this article, you should be able to...
1. Identify the key components and techniques involved in prolonged exposure therapy (PE) for post-traumatic stress disorder (PTSD).
2. Understand four therapeutic approaches and skills utilized in trauma-focused cognitive-behavioral therapy (TF-CBT) for individuals with PTSD.
3. Describe the therapeutic process and unique features of eye movement desensitization and reprocessing (EMDR) in the treatment of PTSD.
Psychotherapy is generally considered to be the treatment of choice for PTSD. There are several evidence-based therapies to choose from. These include prolonged exposure (PE), trauma-focused cognitive behavioral therapy (TF-CBT), cognitive processing therapy (CPT), and eye movement desensitization and reprocessing (EMDR). In this article, I’ll give you a brief overview of each technique.
Prolonged exposure (PE) involves facing and processing traumatic memories and trauma-associated situations in a safe and supportive environment. The technique starts with psychoeducation and brief relaxation training through breathing, and quickly moves into two types of exposure therapy: imaginal and in-vivo exposure to the trauma memories or trauma associated stimuli (Forman-Hoffman et al. Psychological and Pharmacological Treatments for Adults With Posttraumatic Stress Disorder: A Systematic Review Update. May 2018: Comparative Effectiveness Review, No. 207). Like exposure therapy for other anxiety disorders, PE for PTSD involves facing the feared stimulus over and over until anxiety subsides, a process known as habituation.
In imaginal exposure, clients tell their story (called their trauma narrative) to the therapist over and over, adding details each time and reporting their level of distress throughout the exposure. Following the imaginal exposure, the client verbally processes thoughts and feelings that emerged. Clients also listen to a recording of their trauma narrative between therapy sessions. In
in vivo exposure, the client faces real-world reminders of the trauma. For example, a person who has been through a near-fatal car accident and feels terrified at the idea of driving again may sit in a car, then ride in a car driven by someone else, then drive their car up and down the driveway, and finally drive the car on real roads, starting with quiet roads and progressing to other driving situations. It’s important to ensure safety and comfort when guiding clients through these kinds of exercises. PE generally involves eight to 16 therapy sessions lasting 60–90 minutes.
Trauma-Focused Cognitive Behavior Therapy (TF-CBT) shares the exposure components of PE but starts with a more extensive period of psychoeducation, relaxation training, and skills training in cognitive restructuring and emotion regulation. This allows the client to reach a more stable place emotionally before starting the often taxing process of exposure therapy, and also addresses some of the cognitive distortions common in individuals after a trauma (eg, thinking that they caused the traumatic event in some way). TF-CBT generally takes 12–16 weeks and can be done in either individual or group settings.
Cognitive Processing Therapy (CPT) is a therapeutic approach that helps individuals with PTSD to better handle distressing thoughts and feelings associated with their traumatic experiences (Resnick PA et al, Behav Ther. 2024;55(6):1205-1221). Imagine a patient named Maria who has PTSD after a severe car accident. In the initial stages of CPT, the therapist would educate Maria about her specific PTSD symptoms such as flashbacks, avoidance behaviors, and sleep disturbances. They'd also discuss how CPT can address these symptoms.
Next, Maria would be guided to become more aware of the impact of her car accident. She would explore not just the event itself, but also her thoughts and feelings about herself, other people, and the world around her since the incident. For instance, she might realize she has developed a fear of not just driving, but also being a passenger in cars, which has isolated her from family and friends.
The therapist then teaches Maria techniques to identify, challenge, and alter unhelpful thoughts or "stuck points." Maria may have become stuck on the thought that she could have prevented the accident if she had been more vigilant. With CPT, she learns to challenge this belief and understand that she was not at fault for the unpredictable behavior of the other driver.
Maria would be given the choice to write about her traumatic event in detail - this version of CPT is known as CPT+A. Regardless of whether she chooses to do this, the therapy would be effective. Maria, for example, might decide to write her trauma account to help her confront and understand her experience better. In the final stages of CPT, Maria would continue practicing these skills to challenge any altered belief systems. This could include unrealistic beliefs about safety (believing all cars are dangerous), trust (believing all drivers are reckless), control (believing she has no control over her life), self-esteem (believing she is a bad driver), and intimacy (believing no one can understand her experience).
Initially, CPT was designed as a 12-session protocol. However, it's now tailored to each patient's needs. Maria, for instance, might need additional sessions due to the severity of her PTSD symptoms or her difficulty in challenging certain stuck points.
 Eye Movement Desensitization and Reprocessing (EMDR) is a unique therapeutic approach that combines talk therapy with bilateral stimulation, commonly using eye movements, but also tactile or auditory stimuli. It's rooted in the understanding that traumatic memories are stored differently in the brain compared to non-traumatic ones, and that the techniques employed in EMDR can aid the brain in processing these traumatic memories in a healthier, more adaptive manner.
Eye Movement Desensitization and Reprocessing (EMDR) is a unique therapeutic approach that combines talk therapy with bilateral stimulation, commonly using eye movements, but also tactile or auditory stimuli. It's rooted in the understanding that traumatic memories are stored differently in the brain compared to non-traumatic ones, and that the techniques employed in EMDR can aid the brain in processing these traumatic memories in a healthier, more adaptive manner.
Let's consider a patient, David, who is struggling with PTSD after a military combat experience. During a typical EMDR session, David is asked to focus on a specific traumatic memory - perhaps a particularly intense firefight - while concurrently paying attention to an external stimulus, often a moving object or light that the therapist directs. As David recalls his traumatic experience, the therapist guides him through repeated cycles of bilateral stimulation. This could involve following a moving object with his eyes or feeling alternating taps on his hands. Meanwhile, he's encouraged to observe any changes in his emotions, mental images, or insights associated with the memory.
The goal of EMDR is to continue this reprocessing until David can recollect the traumatic memory without the associated distress. He should reach a point where he holds a positive self-belief that feels genuine - for example, instead of feeling like a victim of his traumatic past, he recognizes his strength and resilience as a survivor. Research shows that EMDR can effectively reduce PTSD symptoms. However, the exact mechanism by which it accomplishes this remains an active area of study (Forbes D et al, J Trauma Stress 2010;32(6):783-794).
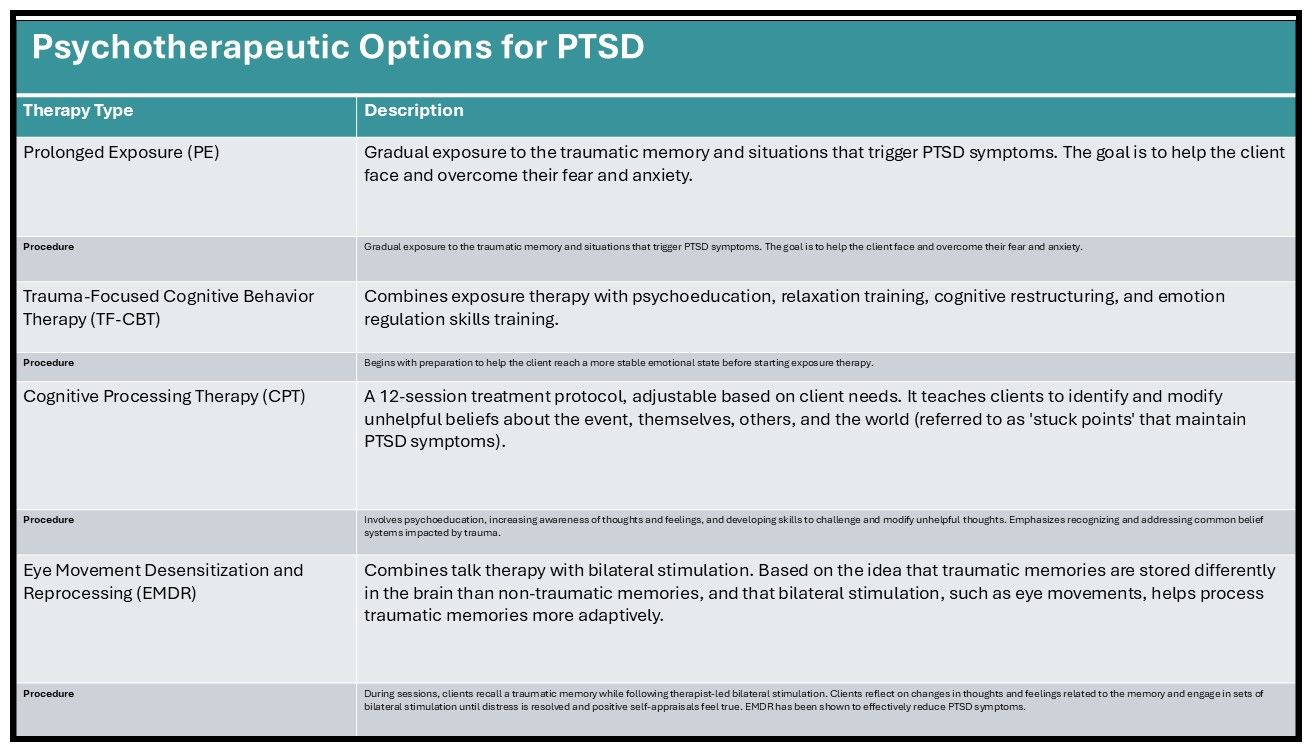
Different clients may respond better to one treatment than another. For example, clients with single-episode trauma who can tolerate the exposure process will find fast relief from PE. Other clients who are too anxious or dysregulated to tolerate exposure therapy right away (for example those with a lot of suicidal thoughts or self-harm), or those who have prominent dissociative symptoms, are likely to have a hard time with PE and should instead be treated with TF-CBT, EMDR, or other treatments that focus on affect regulation skills (McLean CP and Foa EB, Expert Rev Neurother 2011;11(8):1151-1163)(PDF)(For a quick visual, see the table, "Psychotherapeutic Options for PTSD"),
CARLAT VERDICT
Clinicians have several effective, evidence-based psychotherapies for PTSD, each with distinct approaches. Matching the therapy to the patient’s needs and readiness for exposure-based work is key to promoting engagement, emotional processing, and long-term recovery.
References in the order of appearance of this article
Resick, P. A., LoSavio, S. T., Monson, C. M., Kaysen, D. L., Wachen, J. S., Galovski, T. E., Wiltsey Stirman, S., Nixon, R. D. V., & Chard, K. M. (2024). State of the Science of Cognitive Processing Therapy. Behavior therapy, 55(6), 1205–1221. https://doi.org/10.1016/j.beth.2024.04.003.
Forbes, D., Creamer, M., Bisson, J. I., Cohen, J. A., Crow, B. E., Foa, E. B., Friedman, M. J., Keane, T. M., Kudler, H. S., & Ursano, R. J. (2010). A guide to guidelines for the treatment of PTSD and related conditions. Journal of traumatic stress, 23(5), 537–552. https://doi.org/10.1002/jts.20565.
McLean, C. P., & Foa, E. B. (2011). Prolonged exposure therapy for post-traumatic stress disorder: a review of evidence and dissemination. Expert review of neurotherapeutics, 11(8), 1151–1163. https://doi.org/10.1586/ern.11.94.



Recommended


