
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Clinical Update
Negative Symptoms of Schizophrenia
A 56-year-old man with schizophrenia presents for possible depression, but on closer examination has prominent negative symptoms of schizophrenia. When asked about his relationships, he says he keeps to himself and has no friends (asociality). He spends most of the day in a recliner and has trouble starting simple activities (avolition). He speaks in short, five-word sentences (alogia). Although his brother died recently, he speaks of the loss with minimal facial expressions, matching his monotonic voice (blunted affect). He does, however, enjoy documentaries on the “mysteries of the pyramids,” so he lacks the negative symptom of anhedonia.
Negative symptoms like these are part of the core criteria of schizophrenia and are the main cause of disability in this illness. Many treatments have the potential to help, and in this article, we’ll highlight the ones that are ready for practice.
Differential diagnosis
The first step is to rule out a variety of other potential causes of negative symptoms.
Is psychosis the cause?
Symptoms that appear to be negative symptoms can be due to the psychosis itself. In the case above, if the patient heard voices telling him not to leave his recliner, we’d start by treating the active psychosis.
Comorbid conditions
Next, address comorbidities that might be contributing to the picture, like depression, PTSD, substance use, insomnia, and sleep apnea.
Antipsychotic side effects
Antipsychotic side effects can resemble negative symptoms, such as sedation, muscle stiffness, parkinsonian slowing, and amotivation.
Antipsychotics
It is difficult to know for sure whether antipsychotics directly improve negative symptoms, versus improving them only indirectly through treatment of active psychosis. We need trials that test antipsychotics in patients who have recovered from psychosis but continue to experience prominent negative symptoms, and so far we have only a few.
One study compared risperidone to cariprazine in patients who continued to have negative symptoms after recovering from a psychotic episode. The results favored cariprazine, though the benefit was small, with a number needed to treat of 9 (Németh G et al, Lancet 2017;389(10074):1103–1113). Another large trial found favorable results with amisulpride, a European antipsychotic that may come to the US market in the next few years (Krause M et al, Eur Arch Psychiatry Clin Neurosci 2018;268(7):625–639).
Another possibility is clozapine. Although its effects on negative symptoms are not well researched, this medication does bring about higher rates of functional recovery (Kim S et al, Psychiatry Investig 2021;18(10):968–976). Compared to other antipsychotics, clozapine had the largest effect size (0.6) for reducing negative symptoms when used during active psychosis, according to a meta-analysis (Huhn M et al, Lancet 2019;394(10202):939–951). Next in line after clozapine were amisulpride, olanzapine, asenapine, and perphenazine.
Augmentation
Another option is to augment the antipsychotic, and an antidepressant is a reasonable place to start. Studies of SSRIs have been generally positive, though the benefits are small. On the other hand, duloxetine (Cymbalta), mirtazapine (Remeron), and vortioxetine (Trintellix) have yielded larger effect sizes for negative symptoms, although the studies supporting them are still small in size and few in number (Moazen-Zadeh E et al, J Psychopharmacol 2020;34(5):506–513).
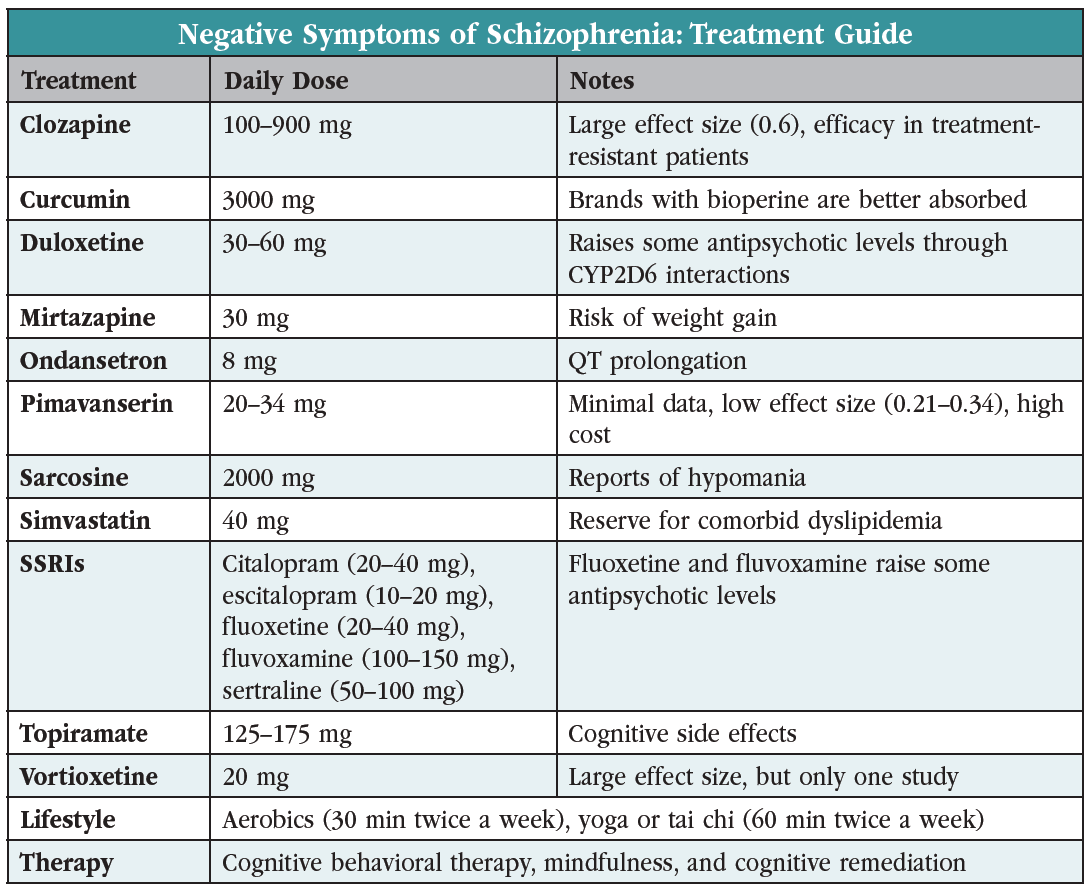 Other augmentation options with positive controlled trials are listed in the table “Negative Symptoms of Schizophrenia: Treatment Guide.” None stand out as more effective, and all are hindered by small effect sizes (0.2–0.3) and small trials. They include simvastatin, minocycline, 5-HT3 inhibitors (ondansetron, granisetron, tropisetron), lamotrigine, and topiramate, as well as augmentation with the novel antipsychotic pimavanserin (Nuplazid). To choose among them, aim for one that addresses active comorbidities, such as simvastatin for dyslipidemia or ondansetron, which has positive trials in OCD and in binge drinking.
Other augmentation options with positive controlled trials are listed in the table “Negative Symptoms of Schizophrenia: Treatment Guide.” None stand out as more effective, and all are hindered by small effect sizes (0.2–0.3) and small trials. They include simvastatin, minocycline, 5-HT3 inhibitors (ondansetron, granisetron, tropisetron), lamotrigine, and topiramate, as well as augmentation with the novel antipsychotic pimavanserin (Nuplazid). To choose among them, aim for one that addresses active comorbidities, such as simvastatin for dyslipidemia or ondansetron, which has positive trials in OCD and in binge drinking.
It may be surprising to see topiramate on this list. This anticonvulsant’s reputation for impairing cognition has earned it the nickname “Dopamax,” but negative symptoms involve more than cognition. Topiramate improved negative and positive symptoms in small trials of treatment-resistant schizophrenia, usually as an add-on to clozapine. Its cognitive side effects are reduced by starting low (25 mg/day) and raising slowly (by 25 mg/week). Patients with comorbid obesity, PTSD, OCD, or alcohol or cocaine use disorders may find additional benefits with topiramate (Correll CU et al, JAMA Psychiatry 2017;74(7):675–684).
Supplements
Most supplements have mixed results for negative symptoms, but two with steadier track records are sarcosine and curcumin. Sarcosine is a sweet-tasting amino acid that is sold as a nootropic. It has multiple small trials showing a moderate benefit for negative symptoms (Strzelecki D et al, Hum Psychopharmacol 2021;36(3):e27770; Singh S and Singh V, CNS Drugs 2011;25(10):859–885). Curcumin is an extract of the turmeric spice that now has two small trials showing benefits (Hosseininasab M et al, J Clin Psychopharmacol 2021;41(1):25–30). Curcumin also has positive trials in depression and in cognitive problems due to various causes. Both of these supplements have evidence in primary negative symptoms, and both are well tolerated, although there are reports of hypomania on sarcosine.
Exercise
Exercise improves primary negative symptoms in schizophrenia, but only in studies of aerobic exercise, and the effect size is small at 0.31 (Sabe M et al, Gen Hosp Psychiatry 2020;62:13–20). “Aerobic” means any activity that hastens breathing and raises pulse by at least 10 bpm. The minimum dose is 30 minutes twice a week over six months. If aerobic exercise is too strenuous, mind-body exercises like yoga or tai chi for two hours a week may also help (Sabe M et al, Schizophr Res 2019;212:15–25). These are challenging prescriptions to follow when a patient suffers from significant amotivation. Recruiting friends or family for dual participation is often necessary.
Psychotherapy
Psychotherapies (specifically cognitive behavioral therapy for psychosis, acceptance and commitment therapy, and metacognitive therapy) show small benefits for primary negative symptoms (Lutgens L et al, Br J Psychiatry 2017;210:324–332). Cognitive remediation is an even better treatment option, with the most rigorous trials improving negative symptoms with a medium effect size (Cella M et al, Clin Psych Rev 2017;52:43–51). This makes intuitive sense as it focuses directly on improving cognitive functioning.
TMS
Neuromodulation techniques are the latest to show promise in negative symptoms. Repetitive transcranial magnetic stimulation (rTMS) brought improvements in several randomized controlled trials (Tseng PT et al, JAMA Psychiatry 2022;79(8):770–779). Insurance is unlikely to cover off-label use of rTMS, and other neuromodulation options with potential benefits (eg, high-definition transcranial random noise stimulation, anodal transcranial direct current stimulation) are not yet clinically available.
CARLAT VERDICT
To treat negative symptoms, start with an antipsychotic that has evidence to help this disabling phase of schizophrenia,particularly cariprazine and possibly olanzapine, asenapine, perphenazine, or—for treatment-resistant cases—clozapine. Next, try augmentation, either with an antidepressant (duloxetine or vortioxetine) or one of the options in the table that addresses the patient’s comorbidities.



Recommended


