
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Expert Q&A
End-of-Life Discussions With Patients With Advanced Dementia
 Ruth Palan Lopez, PhD, GNP, FAAN. Jacques Moore Endowed Professor of Gerontologic Nursing; Associate Dean for Research in the School of Nursing, MGH Institute of Health Professions, Boston, MA.
Ruth Palan Lopez, PhD, GNP, FAAN. Jacques Moore Endowed Professor of Gerontologic Nursing; Associate Dean for Research in the School of Nursing, MGH Institute of Health Professions, Boston, MA.
CGPR: Please tell us about your background and how it motivates your research.
Dr. Lopez: I am a gerontologic nurse practitioner and have provided care to older adults in multiple settings for many years. I became distressed by the way we care for older adults with advanced dementia, specifically in nursing homes. Some patients receive comfort care and palliative interventions, while other patients receive burdensome or painful interventions like frequent transfers to the hospital, feeding tubes, and antibiotics, which we know don’t often benefit them (Lacey D, Am J Alzheimers Dis Other Demen 2005;20(4):211–219). My research focuses on how we can promote comfort for people with advanced dementia at the end of life, whether through palliative care or hospice.
CGPR: What is the difference between palliative care and hospice?
Dr. Lopez: Palliative care is the provision of care that aims to maintain quality of life and relieve suffering. It takes a holistic approach: physical, emotional, and spiritual. It can be delivered at any stage of the disease trajectory and in any setting. Hospice is a type of palliative care for patients generally expected to live six months or less. The Hospice Medicare Benefit is a program established by the United States government to provide Medicare beneficiaries who are terminally ill with comprehensive care that focuses on improving the quality of their remaining life, rather than trying to cure their condition. Hospice care is usually provided at home, in a nursing home with hospice care, or in a specialized hospice facility.
CGPR: You studied the care provided to nursing home residents with advanced dementia in diverse settings (Lopez RP et al, JAMA Intern Med 2022;182(3):313–323). Can you tell us about this study?
Dr. Lopez: There are disparities in end-of-life care by region and race due to systemic discrimination. Black nursing home residents have higher rates of tube feeding and hospital transfers than White residents. Southern regions have higher intervention rates than the North. Our study aimed to understand racial and regional differences in care practices and their impact on end-of-life interventions. We conducted qualitative observations and interviews in regions with varying rates of feeding tube use and hospital transfers. Regardless of geography, staff held a bias that Black family members desired intensive care, resulting in fewer conversations about advance directives, comfort care, or limiting invasive procedures. However, proxies expressed a desire for staff assistance in decision-making. This is in line with research showing that due to a host of systemic discriminatory factors, racially/ethnically minoritized residents are less likely to complete advance directives; they also experience more pain and are more likely to have poor symptom management at the end of life (Estrada LV et al, J Am Med Dir Assoc 2021;22(2):279–290.e1).
CGPR: You also studied the issue of trust in nursing homes. Can you tell us more?
Dr. Lopez: We found what we call “differential trust” (Rogers AH et al, Geriatr Nurs 2021;42(6):1362–1366). Family members trusted staff differently, which is driven by anti-Black medical racism. We found that White family members trusted the predominantly White administration while being less trustful of the predominantly Black direct care workers. We saw the opposite among Black proxies, who tended to trust Black direct care workers but were less trustful of the predominantly White administrators.
CGPR: How can clinicians use this information to improve end-of-life care?
Dr. Lopez: Everyone deserves holistic, person-centered care based on respect for human dignity. Taking time to create trust and improve communication can go a long way. To build trust with the minoritized, we need to explicitly name racism as the driver of inequity and mistrust. Clinicians can also be trained to recognize and address their own biases, including in end-of-life decision-making. We can develop culturally sensitive educational materials that depict diverse cultural perspectives on health care decision-making, treatment options, and end-of-life care. We can also identify and train staff, including case managers and social workers, to meet with residents and their families to discuss health care options, explain medical terminology, and clarify any doubts or concerns they may have. Trained staff may also help residents and their families understand the importance of shared decision-making and can empower residents to actively participate in making health care choices.
CGPR: How else might we change our end-of-life approach based on your findings?
Dr. Lopez: As a result of racism, Black older adults are more likely to be in nursing homes with lower staffing and lower quality of care than White older adults. The solution is to dismantle factors causing minoritization in long-term care facilities. This requires resources and support. In addition, clinicians can consider implementing standardized protocols and guidelines for advance care planning to help ensure that all residents have equal opportunities to discuss and document their end-of-life care preferences. Nursing homes can implement regular monitoring and quality improvement efforts to assess and address disparities in end-of-life care. This may involve analyzing data on advance directive completion rates, pain management, symptom control, quality of life, and family satisfaction.
CGPR: We’ve talked about more system-wide solutions; now let’s turn toward the individual patient and their family members. Can you talk a bit about how health care proxy guilt can affect end-of-life decisions?
Dr. Lopez: It’s interesting—in our research, we found that nursing home staff thought family members felt guilty for not being there when their loved ones were passing away. Staff thought this guilt might affect the choices made by family members. But when we talked to the proxies, the guilt they felt was mostly about having to put their loved ones in the nursing home in the first place. Making choices for a loved one at the end of their life is challenging. Some view it as a duty, while others consider it an honor (Roach A et al, J Gerontol Nurs 2022;48(1):22–27).
CGPR: What can clinicians do to minimize guilt and feelings of excessive responsibility in proxies?
Dr. Lopez: Framing difficult decisions as a choice between prolonging life or withholding care may not accurately reflect the situation. I have had many conversations with family members who feel that they hastened or contributed to their loved one’s death when they chose comfort over “life prolongation.” Some family members who participate in end-of-life decision-making also experience posttraumatic stress disorder (Gries CJ et al, Chest 2008;133(3):704–712). As proxies often want assistance from clinicians in making end-of-life decisions, clinicians can initiate conversations, provide information about comfort-focused care options, and offer guidance based on evidence-based practices, such as effective pain management and symptom control (Morrison RS et al, JAMA 2021;326(16):1575–1576).
CGPR: How do we assess what makes patients with dementia most comfortable?
Dr. Lopez: Some readers may have heard about the Age-Friendly Health System, which is a movement to improve health care in older adults. This model of care suggests that clinicians focus on the 4Ms at every visit with an older adult: what matters, medications, mobility, and mentation. I adapted these 4Ms for people with advanced dementia, by adding “mealtimes” and “make comfortable,” and changing mentation to “meaningful activities,” to make 6Ms (Lopez RP et al, J Gerontol Nurs 2023 [in press]).
CGPR: Tell us more about evaluating the 6Ms.
Dr. Lopez: To prioritize what matters, we ask about advanced directives, preferred names, significant family members, and notable achievements. We identify meaningful activities—what makes them smile now. We discontinue medications and procedures that no longer provide benefit, such as lipid-lowering drugs, vitamins and supplements, or routine blood draws. We ensure comfortable mobility and identify their favorite places. During mealtimes, we address swallowing difficulties by offering preferred foods, modifying consistency, and finding optimal feeding positions. When it comes to making a patient comfortable, we rely on nonverbal cues and deliver daily care with sensitivity. For example, we may assess whether they prefer a bath, towel bath, or shower (Editor’s note: See “The 6Ms of Caring for People With Advanced Dementia” table).
CGPR: Any tips for navigating a patient’s end-of-life choices when they are influenced by depression?
Dr. Lopez: That’s difficult because we are influenced by ageism. If a young person is depressed and doesn’t want to eat anymore, clinicians investigate and treat their depression, and hopefully the patient’s appetite improves. When an older person refuses to eat, our ageism tends to make us overlook their depression, and we are less likely to treat it. I think clinicians should investigate depression regardless of age, and it should be treated regardless of age.
CGPR: While talking about end-of-life issues can be painful, families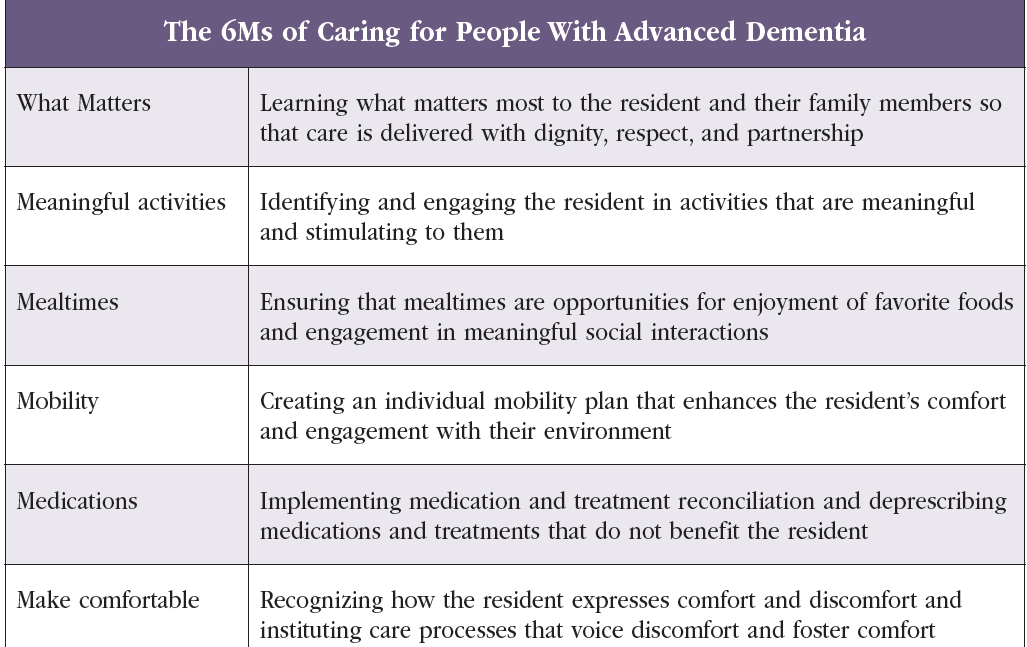 appreciate the opportunity to be heard. Are there any practical limitations to person-centered care?
appreciate the opportunity to be heard. Are there any practical limitations to person-centered care?
Dr. Lopez: Clinicians should consider whether staff can deliver a care plan based on a patient’s preferences. For example, a patient’s wish to walk outside may be limited by staffing, or eating foods that greatly increase a patient’s risk for choking may not be feasible. A major limitation is that individuals with advanced dementia cannot verbalize their preferences. Therefore, clinicians must rely on care partners to learn about their values, preferences, and personhood. To overcome this barrier, we need to empower care partners to engage with us and provide this crucial information.
CGPR: What tips do you have for communicating with patients and their caregivers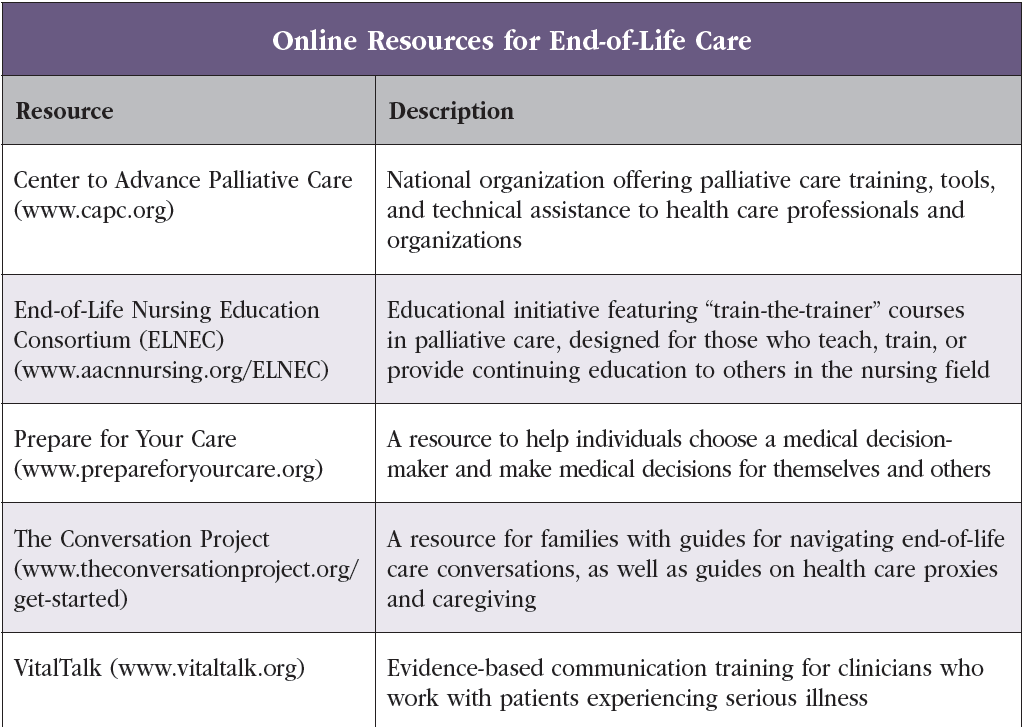 about end-of-life care preferences?
about end-of-life care preferences?
Dr. Lopez: Be confident and communicate directly. Although we don’t want to hurt people’s feelings, scare them, or take away hope, we shouldn’t dance around the issues. You can use words like “dying.” I like to say: “Advanced dementia is the last chapter of life. How do you want to write this chapter?” I also share my belief that it is critically important for the person who is dying to experience comfort—not to experience undue, invasive, painful procedures at the end of life, especially procedures in which families are rushed out of the room and unable to sit and hold hands and be together. I’m clear that life prolongation is not an achievable goal. I tell patients and families that CPR doesn’t bring people with advanced dementia back to life in any meaningful way. It may restart the heart, but it will not stop the dementia. I say that I have no control over the quantity of life, but I can help work with the quality of that life—how to keep people free of pain, anxiety, and distress.
CGPR: Clinicians often experience discomfort in discussing end-of-life planning. What resources do you recommend to improve their comfort level?
Dr. Lopez: Discussing end-of-life planning can be a difficult and emotionally challenging topic for clinicians. However, it is an essential part of providing quality care to patients, especially those with advanced or serious illnesses. Resources that clinicians can use include communication tools, peer support and mentoring, personal reflection, and self-care (Editor’s note: See “Online Resources for End-of-Life Care” table).
CGPR: Thank you for your time, Dr. Lopez.


Recommended


