
_-The-Breakthrough-Antipsychotic-That-Could-Change-Everything.webp?t=1729528747 "KarXT (Cobenfy)_ The Breakthrough Antipsychotic That Could Change Everything.jpg")
Clinical Update
Sexual Health in Older Adults: A Primer
Sexuality is a broad term that encompasses sexual identity, activity, attitude toward sex, intimacy, partnership, and pleasure. In this article, we cover the basics of sexual function and the effects of aging, medical comorbidities, and mental health on sexuality. We discuss sexual health in long-term care settings and in older adults with cognitive disorders and suggest an approach to commonly encountered sexual health issues.
Assessing sexual health in older adults
Older adults are sexually active, but sexual issues are often not discussed in health care settings. This may be due to patient or clinician discomfort, lack of knowledge, fear of embarrassment, or ageist beliefs (Srinivasan S et al, Curr Psychiatry Rep 2019;21(10):97). However, a healthy sex life is integral to the quality of life for many older adults. To assess sexual activity, I generally start by asking for permission to discuss sexuality with the patient. I then ask open-ended questions such as “What concerns or questions do you have in terms of your sexual activity?” I may also ask “Have you noticed changes in your sexual relationship with your partner over time?” Many older adults will not disclose sexual health issues if there are others in the room, so I try to ensure privacy when screening for sexual dysfunction. I ask about problems with libido, getting/maintaining an erection (for men), dryness or discomfort (for women), and difficulty achieving orgasm (for both). I also ask whether they have concerns about their partner’s sexual health. For patients at risk, I recommend screening for sexually transmitted diseases. To minimize patient discomfort, I ask questions in a respectful, open-ended, but matter-of-fact manner. This allows patients to feel more comfortable sharing any other concerns they might have. I don’t assume heterosexual/monogamous relationships, allowing patients to disclose their sexual preferences as they are comfortable.
Medical comorbidities
In patients with sexual dysfunction, I always ask about medical comorbidities. Parkinson’s disease, cancer, diabetes, and coronary artery disease can cause sexual dysfunction (Slack P and Aziz VM, BJPsych Advances 2020;26(3):173–182). I then tailor treatment recommendations to the underlying causes. I may recommend medications like sildenafil, referral to urology or sexual health counseling, or evaluation for pelvic floor physical therapy.
Medication side effects
Depression and anxiety are important risk factors for sexual dysfunction, as are the medications used to treat them. SSRIs can cause hypoactive sexual desire, erectile dysfunction, and delayed ejaculation (Slack et al, 2020). I routinely discuss sexual side effects both prior to prescribing antidepressants and on the first few follow-ups after starting a new medication. Side effects are often dose dependent and usually reversible, but they can persist after discontinuation. I sometimes recommend brief drug holidays for 24–48 hours prior to planned sexual activity. I may also switch to antidepressants less likely to cause sexual side effects, such as bupropion, mirtazapine, or vortioxetine.
Antipsychotics can reduce libido and cause erectile dysfunction and amenorrhea. First-generation antipsychotics and “prolactin-inducing” antipsychotics, such as risperidone and paliperidone, have more sexual side effects. I typically screen for sexual side effects at the first follow-up visit after starting an antipsychotic. For patients who develop sexual side effects, I may switch to aripiprazole, which has fewer sexual side effects, or I may recommend use of adjuvant sildenafil to reduce sexual dysfunction.
Treating sexual dysfunction
Sexual dysfunction increases with age. Women have lower estrogen levels after menopause, which may cause vulvovaginal atrophy and pain during intercourse. In older women experiencing sexual discomfort, I may recommend using vaginal lubricants. I often encourage women to discuss treatment options, including local and systemic hormone therapy, with their primary care physician. In older men experiencing erectile and ejaculatory dysfunction, I first let them know that their condition is common. Depending on the needs of the patient, I may discuss how to manage modifiable risk factors such as obesity, smoking, or hypertension. I may also recommend psychotherapy or a trial of a phosphodiesterase-5 inhibitor.
Treating inappropriate sexual behavior in dementia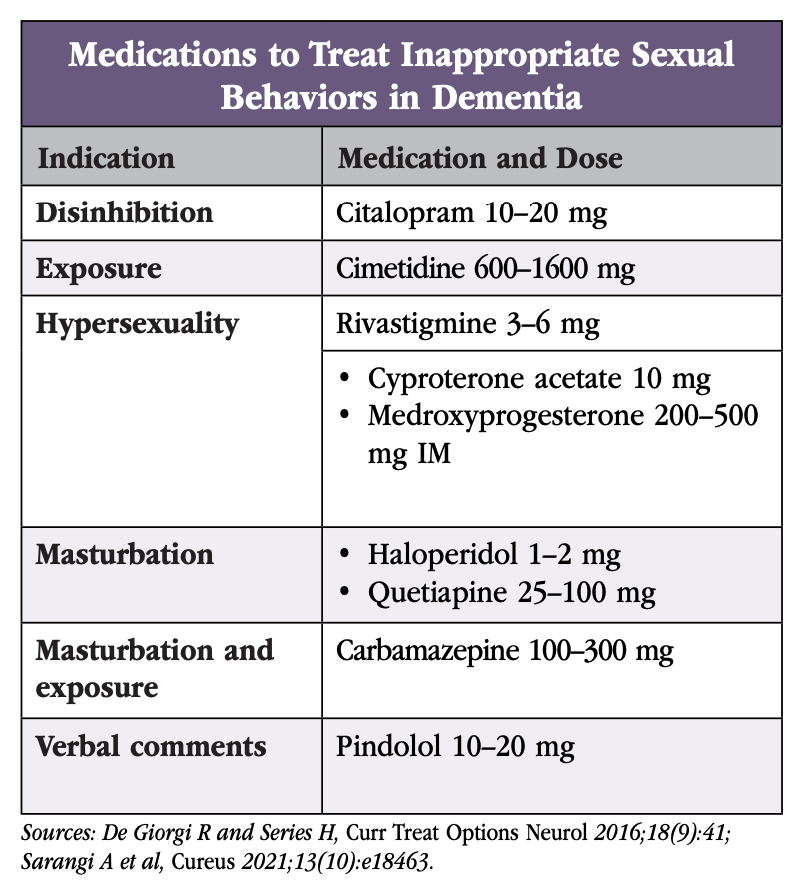
Indifference to sexual activity is common in Alzheimer’s dementia, though disinhibited behaviors receive more attention. Sexual disinhibition can present early in frontotemporal dementia and during later stages in other dementias. There is a lack of good evidence for the use of psychotropics to address inappropriate sexual behaviors. Rather, behavioral interventions such as redirection, distraction, and reminders are more effective. Clothing such as jumpsuits and shirts with buttons in the back are sometimes used to prevent exposure, but clinicians may consider weighing the risks and benefits to determine whether this is necessary.
If behavioral interventions are not sufficient to reduce inappropriate sexual behaviors, case studies support the use of antidepressants, especially SSRIs, as well as antipsychotics (Black B et al, J Geriatr Psychiatry Neurol 2005;18(3):155–162). There is weak evidence for the use of mood stabilizers, antihypertensives, and cimetidine. Although clinicians may consider anti-androgens (cyproterone acetate) and progestins (medroxyprogesterone), these are rarely used due to ethical concerns when prescribed to patients who lack the capacity to consent to treatment. (See table for a breakdown of medications and dosages.)
Table. Medications to Treat Inappropriate Sexual Behaviors in Dementia.
Click to view the PDF
Sexuality in long-term care
There are many barriers to healthy sexual expression in long-term care settings, including but not limited to:
- Staff bias (eg, labeling sexual behaviors as “inappropriate”)
- Lack of privacy
- Practice of separating couples upon entrance to long-term care
- Concerns about consent and capacity
- Discrimination against LGBTQ adults
Risk and capacity assessment training may increase staff confidence in managing sexual behaviors and in creating spaces for residents to safely express their sexuality. Additionally, changing the environment, such as providing Do Not Disturb signs and private spaces, can make long-term care residents feel more comfortable.
Patients identifying as LGBTQ
There are high levels of discrimination against patients identifying as LGBTQ, including in long-term care settings. Older adults identifying as LGBTQ often internalize this stigma and may be reluctant to engage in conversations about sexuality. Adults identifying as LGBTQ often prefer to age in place and delay entry into long-term care settings due to concerns about stigma and autonomy, as well as fear of abuse due to their sexual orientation (Schwinn SV and Dinkel SA, Online J Issues Nurs 2015;20(2):7). Staff training and education can counter this stigma. Clinicians can also help by not making assumptions about the sexual preferences of older adults. Rather, they can ask open-ended questions about sexual preferences using inclusive language. Clinicians may also assist older LGBTQ adults in finding resources in their community, such as through the Services and Advocacy for LGBT Elders USA website (www.sageusa.org).
CARLAT VERDICT
Sexuality can be an important part of life for older adults, and sexual dysfunction is common. Patients often benefit when clinicians ask about their sexual health, as treatment of sexual dysfunction can improve a patient’s quality of life. Treatments include behavioral interventions, psychotherapy, and medications.


Recommended


